
Un cas rare d’une péritonite hématologique compliquant une myélofibrose secondaire.
DOI :
https://doi.org/10.25796/bdd.v8i3.87085Mots-clés :
dialyse péritonéale, péritonite, dialysat trouble, péritonite à culture négative, myélofibrose secondaireRésumé
La péritonite est l’une des complications fréquentes de la dialyse péritonéale. Son diagnostic repose sur des signes cliniques (douleur, effluent trouble), une hyperleucocytose intrapéritonéale (> 0,1×109/L avec plus de 50 % de polynucléaires), et/ou une culture positive. Bien que la majorité des péritonites soient d’origine infectieuse, il existe des formes d’origine non infectieuse qui peuvent entrainer un usage inapproprié d’antibiotiques et un retard diagnostic. Nous rapportons le cas d’un patient de 78 ans, atteint d’une hémopathie complexe qui associait hémoglobinurie paroxystique nocturne, malgré un traitement par ravulizumab, et une thrombocytémie essentielle transformée en myélofibrose. Après initiation d’un traitement par dialyse péritonéale, il a présenté un liquide de dialyse parfois trouble et riche en leucocytes (jusqu’à 0,442 ×109/L), aucune infection n’a été mise en évidence (cultures et PCR ADN16S négatives, CRP modérée, absence de cellules atypiques). L’origine de l’hyperleucocytose intra-péritonéale a été attribuée à l’hyperleucocytose sanguine liée à la myélofibrose. L’évolution clinique a été défavorable, menant à une prise en charge palliative.
Ce cas illustre la difficulté de la prise en charge de cette complication chez les patients en dialyse péritonéale. Bien que le diagnostic de première intention, par argument de fréquence, soit la péritonite infectieuse, il parait nécessaire d’évoquer les différents diagnostics différentiels en cas de péritonite à culture négative et notamment les différentes causes hématologiques (leucémies, lymphomes, myélofibrose). Cependant, les formes avec prédominance de polynucléaires neutrophiles dans le dialysat peuvent simuler une infection. L’absence de fièvre, de CRP élevée, et une corrélation entre hyperleucocytose sanguine et péritonéale devraient aider au diagnostic différentiel. L’immunophénotypage ou la biologie moléculaire dans le dialysat pourrait affiner le diagnostic. Ce cas met en évidence une cause possible de péritonite stérile, la myélofibrose avec hyperleucocytose, et invite à adapter les recommandations à des situations cliniques de plus en plus complexes.
INTRODUCTION
La dialyse péritonéale est l'une des techniques de suppléance rénale. Celle-ci est couramment utilisée en France bien qu'en proportion nettement inférieure à l'hémodialyse [1]. Comme toute technique, elle n'est pas dénuée de complications, et la plus connue d'entre elles est la péritonite [2][3].
Le diagnostic de péritonite repose sur la présence d’au moins deux des éléments suivants [4] :
- caractéristiques cliniques compatibles avec une péritonite, c’est-à-dire douleur abdominale et/ou effluent de dialyse trouble ;
- numération des globules blancs dans l’effluent de dialyse > 100/µL ou > 0,1 × 109/L (après un temps de stase d’au moins 2 h), avec > 50 % de leucocytes polymorphonucléaires (PMN) ;
- culture positive des effluents de dialyse.
La majorité des péritonites sont d'origine infectieuse mais il existe d'autres étiologies qu'il est nécessaire d'évoquer et de rechercher [5][6][7][8]. D'une manière globale, les signes de péritonite sont interprétés, en première intention, comme d'origine infectieuse pour éviter le retard de prise en charge pouvant être responsable d'une morbi mortalité importante. Cependant, ceci peut être responsable de plusieurs complications dont une utilisation excessive des antibiotiques avec un risque de modification de l'écologie bactérienne et d'émergence de résistance et/ou un retard de prise en charge de la pathologie incriminée (iatrogénie, allergie, maladie oncologique ou hématologique, pathologie chirurgicale).
De ce fait, les recommandations de prise en charge des péritonites [4] insistent sur la nécessité d'initier rapidement des antibiotiques devant la potentielle gravité de cette infection, mais il est nécessaire de nuancer ces recommandations et d'adapter la prise en charge au cas par cas.
Les patients pris en charge en néphrologie sont souvent âgés, polypathologiques et avec une polymédication importante. Cela nous confronte à différentes complications et/ou observations notamment lors de contextes oncologiques et hématologiques.
Nous rapportons ici un cas de péritonite non infectieuse se manifestant par un effluent de dialyse péritonéale parfois trouble associé à la présence d'un excès de globules blancs intrapéritonéaux secondaire à une hyperleucocytose sanguine, elle-même secondaire à une maladie hématologique.
PRÉSENTATION DU CAS
Un homme de 78 ans a développé une insuffisance rénale chronique stade V dans un contexte d’hémoglobinurie paroxystique nocturne évoluant malgré un traitement par ravulizumab (Ultomiris ®, Alexion Pharma France) puis eculizumab (Soliris ®, Alexion Pharma France). Il avait des antécédents d’hémoglobinurie paroxystique nocturne mais aussi de thrombocytémie essentielle avec diagnostic prouvé en cytogénétique par mutation de MPL W515L et DNMT3A associée, secondairement transformée en myélofibrose traitée par hydroxyurée (Hydrea ®) et ruxolitinib (Jakavi ®) depuis 2023 (avec une hyperleucocytose connue à 30G/L). Il présentait aussi un flutter et de l’hypertension artérielle.
Il a débuté l’épuration extra-rénale en urgence par une technique d’hémodialyse après pose d’un cathéter tunnelisé jugulaire interne droit le 28 octobre 2024, secondairement relayé par la dialyse péritonéale le 6 janvier 2025 (après pose d’un cathéter de dialyse péritonéale accompagnée d’une cure de hernie inguinale le 9 décembre 2024).
Son protocole a comporté un échange court (4h) de solution isotonique (Physioneal 40 ® avec glucose 1,36% ®, Baxter, International Inc) et un échange long de solution hypertonique (Extraneal ®, Baxter, International Inc) sur le reste du nycthémère. Le protocole a été adapté aux besoins du patient, à sa fonction rénale résiduelle mais aussi à la disponibilité des infirmières diplômées d’état libérales pour l’assister à domicile.
Le 13 janvier 2025, les infirmières libérales ont signalé une difficulté de drainage et des douleurs abdominales. Le patient a été pris en charge en hospitalisation de jour avec la réalisation d’un échange retrouvant un liquide de drainage décrit comme clair. Cependant, l’étude cytologique a révélé une numération des globules blancs de 0,139 × 10⁹/L, avec 53 % de polynucléaires. L’analyse sanguine a objectivé une CRP à 8 mg/L, un taux d’hémoglobine à 9 g/dL et une numération leucocytaire à 63 × 109/L, avec 36 × 109/L de polynucléaires. Des prélèvements bactériologiques du liquide de dialyse et sanguins ont été mis en culture. L’ASP a retrouvé un cathéter en place mais avec une accumulation de matières fécales. Dans l’hypothèse d’une péritonite infectieuse liée à la dialyse péritonéale, il lui a été administré un traitement antibiotique empirique par voie intrapéritonéale de Céfazoline et Ceftazidine (selon le protocole de service du CHU de Toulouse). Devant la stabilité clinique, le patient est rentré à domicile.
Le 14 janvier 2025, il est réévalué en consultation devant la persistance des douleurs abdominales et un liquide de drainage légèrement trouble. L’étude cytologique a révélé une numération des globules blancs de 0,197 × 10⁹/L, soit en augmentation, avec 51% de polynucléaires. Il a été hospitalisé dans le service de néphrologie le jour même. L’examen physique à l’admission a montré une apyrexie, une pression artérielle à 160/80 et une fréquence cardiaque à 70 bpm. L’auscultation cardiopulmonaire était normale. L’abdomen était sensible sans défense ni contracture. Les résultats des examens de laboratoire et d’imagerie après l’admission sont les suivants :
- La nouvelle analyse cytologique du liquide de dialyse a révélé une numération des globules blancs de 0,201 × 109/L, avec 29% de polynucléaires,
- La culture de l’effluent s’est révélée négative ainsi que l’ADN16S (ADN bactérien par PCR),
- L’analyse sanguine a révélé une CRP à 4,4 mg/L, un taux d’hémoglobine à 8,7 g/dL et une numération leucocytaire à 67 × 109/L à prédominance de PNN,
- Les hémocultures se sont toutes révélées négatives,
- La tomodensitométrie a retrouvé un épaississement pariétal du colon associé à une infiltration de la graisse péri colique.
Devant l’ensemble des résultats et malgré une absence d’augmentation de la CRP, le diagnostic de colite sans péritonite a été retenu motivant un changement de l’antibiothérapie pour de la Tazocilline par voie intra veineuse pour une durée totale de 7 jours. Le patient est rentré à domicile.
Le 03 février 2025, devant une asthénie persistante, des examens ont été réalisé afin d’évaluer la progression de sa maladie hématologique :
- Le myélogramme a retrouvé une moelle pauvre avec une hypoplasie de la lignée érythroïde, une dysmyélopoïèse modérée, sans excès de blastes,
- Le phénotypage lymphocytaire dans la moelle a montré une absence d’expansion significative des sous-populations lymphocytaires,
- L’analyse en biologie moléculaire des hémopathies a retrouvé la mutation DNMT3A décrite précédemment.
Le 05 février 2025, il a été hospitalisé pour la prise en charge d’une altération de son état général et des saignements spontanés. L’examen physique à l’admission a montré une pression artérielle à 130/60 et une fréquence cardiaque à 70 bpm, apyrétique. L’auscultation cardiopulmonaire était normale. L’abdomen était toujours sensible. Le drainage du liquide de DP a révélé un liquide trouble, sans fibrine. L’analyse du liquide de DP a objectivé une numération des globules blancs de 0,442 × 109 /L, avec 41% de polynucléaires. L’analyse sanguine a révélé une CRP 2.9 mg/L, un taux d’hémoglobine à 10.2 g/dL et une numération leucocytaire à 62 × 109 /L. L’ensemble des cultures se sont révélées négatives. L’évolution de ces paramètres est résumée dans le Tableau I.
| Date | Aspect effluent | GB sang (x109/L) | CRP (mg/L) |
GB effluent (x109/L) |
PNN effluent (en %) |
PNB effluent (en %) |
Lymphocytes effluent (en %) |
Monocytes Macrophages effluent (en %) |
|---|---|---|---|---|---|---|---|---|
| 13/01/2025 | Clair | 63 | 8 | 0,139 | 53 | 1 | 2 | 44 |
| 14/01/2025 | Trouble | NA | NA | 0,197 | 51 | 1 | 3 | 45 |
| 15/01/2025 | Trouble | 67 | 4,4 | 0,201 | 29 | 1 | 7 | 63 |
| 05/02/2025 | Trouble | 62 | 2,9 | 0,442 | 41 | 1 | 2 | 56 |
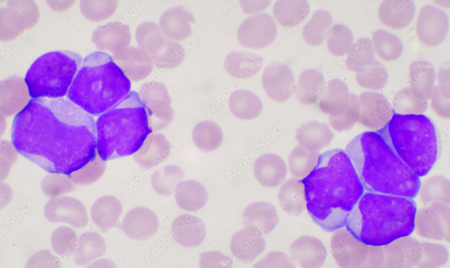
A noter que sur l'ensemble des analyses du liquide de dialyse, il n'a pas été mis en évidence de cellule atypique sur les lames examinées. Nous n'avons pas réalisé de phénotypage dans l'effluent de dialyse étant donné que le phénotypage dans la moelle était normal.
Le diagnostic qui a été retenu est celui d'une évolution au stade terminal de sa maladie hématologique avec hyperleucocytose intrapéritonéale secondaire à l'hyperleucocytose sanguine réfractaire aux traitements médicaux. Cependant, cela reste une hypothèse étant donné que nous n'avons pas réalisé d'analyse en biologie moléculaire sur l'effluent, ce qui aurait pu nous permettre de confirmer la présence de cellules pathologiques avec la mutation précédemment décrite.
L'évolution a été défavorable avec une orientation vers un traitement palliatif.
DISCUSSION
La péritonite infectieuse au cours de la dialyse péritonéale est une complication classique dont la morbi-mortalité spontanément faible, augmente significativement en cas de retard de prise en charge. Les infections péritonéales sont un motif assez fréquent d’arrêt de la technique avec un relais vers l’hémodialyse. En 2018, d’après la RDPLF, 14 % des transferts sont secondaires à une péritonite [9].
D’autre part, la péritonite stérile est un problème courant chez les patients recevant une dialyse péritonéale. Il est donc primordial de savoir diagnostiquer et prendre en charge les différentes causes de péritonite. Les cultures de dialysat péritonéal s’avèrent négatives dans 20% des cas dans de veilles études [10] mais plutôt entre 10 et 15% actuellement (14,6% selon la RDPLF en 2017, 13,7 % au CHU de Toulouse entre 01/01/2020 et 01/01/2025). Dans ces situations, il est primordial d’éliminer en première intention une cause infectieuse difficile à mettre en évidence, comme les mycobactéries, les champignons ou les parasites. Il est alors intéressant de regarder la distribution des différents types de cellules dans l’échantillon de dialysat. Lorsque que celle-ci est à prédominance de polynucléaires neutrophiles, le doute d’une péritonite infectieuse persiste toujours et il est parfois difficile de ne pas poursuivre une antibiothérapie dans l’hypothèse d’une péritonite infectieuse à culture négative.
Cependant, devant la présence de globules blancs à prédominance de polynucléaires neutrophiles et en l’absence de cause infectieuse retrouvée, il est nécessaire de rechercher les autres étiologies [8] :
- L’inflammation des organes intrapéritonéaux (appendicite, cholécystite…),
- L’inflammation des organes rétropéritonéaux (infarctus splénique, abcès splénique, pancréatite…) [11][12][13][14][15],
- Les tumeurs malignes des organes solides (carcinomes rénaux, cancer de l’endomètre…) [16][17][18][19].
Après revue de la littérature, nous avons réalisé un tableau (Tableau II) des étiologies possibles de leucocytose à prédominance de neutrophiles sur le liquide de dialyse péritonéale et à culture stérile.
| CATEGORIE | ETIOLOGIES | PROPOSITIONS |
|---|---|---|
| Infection vraie mais culture négative | Mycobactérie (TB)Champignons (Candida, Aspergillus, Mucormycose)Bactéries fastidieuses (Brucella, Legionella)Anaérobies mal prélevés | Germes difficiles à isoler : cultures prolongées et / ou PCR souvent nécessaires |
| Antibiothérapie préalable | Antibiotiques débutés avant le prélèvement | Fenêtre d’antibiothérapie à discuter |
| Erreur technique | Prélèvement ou transport inadéquatContamination du flacon | Répéter les prélèvements |
| Péritonite chimique | Irritation par antiseptique (iode, chlorhexidine)Rupture de poche de dialyse | |
| Hémopéritoine | Traumatisme secondaire au cathéter avec perforation digestive | Imagerie+/- endoscopie+/- prise en charge chirurgicale |
| Maladie inflammatoire ou auto-immune | Lupus érythémateux disséminéVascularites | |
| Inflammation des organes intrapéritonéaux | AppendiciteCholécystite | Imagerie |
| Inflammation des organes rétropéritonéaux | Pancréatite aiguëAbcès spléniqueInfarctus splénique | ImagerieBiologie (dont lipase / amylase) |
| Tumeur maligne des organes solides / carcinose péritonéale | Carcinomes rénauxCancer de l’endomètreMétastases péritonéalesLymphome | Imagerie+/- biopsie ou exérèse+/- analyse de l’effluent de DP en anatomopathologie, immunophénotypage, biologie moléculaire |
| Rupture d’organe creux | Ulcère perforé, diverticulite, appendicite | Imagerie+/- prise en charge chirurgicale |
| Ischémie | Ischémie mésentérique (occlusion AMS) | Imagerie |
Les causes hématologiques sont, elles, majoritairement retrouvées lorsque le liquide de dialyse est à prédominance de lymphocytes, l’étiologie la plus courante étant le lymphome. Après revue de la littérature, nous avons trouvé 6 cas rapportés de lymphomes diagnostiqués dans le cadre d’une suspicion de péritonite [20][21][22][23][24][25]. L’explication physiopathologique est la présence d’un nombre accru de lymphocytes atypiques secondaire à une diffusion intra péritonéale. Il est donc possible que d’autres maladies hématologiques puissent se compliquer d’une péritonite aseptique. Cependant, nous n’avons pas retrouvé d’autres cas dans la littérature actuelle.
La thrombocytémie essentielle peut dans certains cas se transformer en myélofibrose secondaire.
Les complications de la myélofibrose secondaire peuvent être divisées en 3 groupes :
- Les signes généraux dont l’asthénie, les sueurs et l’hyperthermie,
- La myéloprolifération dont la splénomégalie, l’hyperleucocytose,
- Les cytopénies dont l’anémie et la thrombopénie.
Ces complications évoluent de façon plus ou moins rapide et peuvent donc parfois simuler des tableaux d’infections (notamment l’hyperthermie et l’hyperleucocytose). Dans certains cas, d’importantes hyperleucocytoses sont présentes et ceci est un marqueur de mauvais pronostic avec un risque de résistance au ruxolitinib et d’évolution défavorable de la maladie [26].
Dans ce cas clinique, nous avons recueilli les données cliniques et biologiques d’un patient ayant présenté une péritonite stérile, dans le cadre d’une dialyse péritonéale. Les données recueillies suggèrent que cette péritonite est secondaire à sa maladie hématologique, à savoir une thrombocytémie essentielle avec une myélofibrose secondaire.
Cependant, ce cas clinique montre les limites d’un tel diagnostic en première intention. En effet, il est difficile de ne pas évoquer une péritonite infectieuse devant la présence de leucocytes intra péritonéaux supérieurs au seuil considéré comme pathologique et dont le pourcentage en polynucléaires neutrophiles est supérieur à 50%. D’ailleurs, la première observation du cas était peut-être en lien avec un épisode infectieux digestif et/ou avec une première poussée de sa maladie hématologique. Il est difficile de choisir entre les deux hypothèses. Nous pouvons observer que, par la suite, le liquide de dialyse est plus panaché qu’initialement ce qui nous oriente plus facilement vers une cause hématologique.
Lors d’une suspicion de péritonite hématologique, il pourrait être intéressant de réaliser un immunophénotypage lymphocytaire et/ou une analyse en biologie moléculaire dans l’effluent de dialyse selon la cause suspectée et sa méthode diagnostique. Ceci aurait pu nous aider à la confirmation du diagnostic de péritonite hématologique.
• Pancréatite aiguë Ces résultats montrent que certains marqueurs clinico -biologiques devraient nous sensibiliser à rechercher des diagnostiques différentiels de péritonites infectieuses, et notamment l'apyrexie et l'absence de syndrome inflammatoire biologique associé (CRP). De plus, ils mettent en lumière une nouvelle possible cause de péritonite à culture négative.
CONCLUSION
Cette observation met en lumière un nouveau potentiel diagnostic alternatif à une péritonite stérile. Cela incite à envisager de nouvelles causes de péritonites à culture négative tout en restant vigilant vis-à-vis des péritonites infectieuses qui doivent être évoquées en première intention.
Contributions des auteurs
ChG a contribué à la collecte et l’analyse des données, à la conceptualisation et à la méthodologie de l’étude, ainsi qu’à la rédaction du manuscrit original. HEH a effectué la revue de la littérature et révisé le manuscrit. Tandis que ClG et MBN ont effectué la révision finale et donné leur accord pour la publication.
Financement
Les auteurs n’ont reçu aucun soutien financier pour la recherche, la rédaction et/ou la publication de cet article.
Conflits d’intérêts
Aucun conflit d’intérêt à déclarer.
Considérations éthiques
Conformément aux exigences éthiques, nous précisons que le consentement éclairé n’a pas pu être obtenu, l’étude ayant été conduite de manière rétrospective après le décès du patient.
Identifiants ORCID
Charlotte Gabilan : https://orcid.org/0009-0002-5048-7657
Marie Béatrice Nogier : https://orcid.org/0000-0001-9888-2547
Copyright & License
© © Charlotte Gabilan 2025.
Ce travail est disponible sous la licence Creative Commons Attribution 4.0 International .

Références
1. Réseau REIN. Synthèse du rapport annuel 2022 du réseau REIN [en ligne]. 2022 [cité le 1 mai 2025]. Disponible sur : https://www.agence-biomedecine.fr/fr/observatoire-de-la-maladie-renale-chronique/synthese-du-rapport-annuel-2022-du-rein-par-et-pour-les-patients-presentant-une-defaillance-renale-et-leurs-proches
2. Sahlawi, Muthana Al et al. “Peritoneal dialysis-associated peritonitis outcomes reported in trials and observational studies: A systematic review.” Peritoneal dialysis international: journal of the International Society for Peritoneal Dialysis vol. 40,2 (2020): 132-140. doi:10.1177/0896860819893810
3. Marshall, Mark R. “A systematic review of peritoneal dialysis-related peritonitis rates over time from national or regional population-based registries and databases.” Peritoneal dialysis international: journal of the International Society for Peritoneal Dialysis vol. 42,1 (2022): 39-47. doi:10.1177/0896860821996096
4. Li, Philip Kam-Tao et al. “ISPD peritonitis guideline recommendations: 2022 update on prevention and treatment.” Peritoneal dialysis international: journal of the International Society for Peritoneal Dialysis vol. 42,2 (2022): 110-153. doi:10.1177/08968608221080586
5. Verger C, Veniez G, Dratwa M. Variability of aseptic peritonitis rates in the RDPLF. Bull Dial Domic [Internet]. 2018 Jun. 13 [cited 2022 Sep. 5];1(1):9-13. Available from: https://doi.org/10.25796/bdd.v1i1.30
6. Rocklin, M A, and I Teitelbaum. “Noninfectious causes of cloudy peritoneal dialysate.” Seminars in dialysis vol. 14,1 (2001) : 37-40. doi:10.1046/j.1525-139x.2001.00012.x
7. Teitelbaum, Isaac. “Cloudy peritoneal dialysate: it’s not always infection.” Contributions to nephrology vol. 150 (2006): 187-194. doi:10.1159/000093594
8. Cheng, Xin Bo Justin, and Joanne Bargman. “Complications of Peritoneal Dialysis Part II: Nonmechanical Complications.” Clinical journal of the American Society of Nephrology: CJASN vol. 19,6 (2024): 791-799. doi:10.2215/CJN.0000000000000418
9. Verger C, Fabre E, Veniez G, Padernoz MC. Données statistiques synthétiques du Registre de Dialyse Péritoneale de Langue Française et Hémodialyse à Domicile (RDPLF) en 2018. Bull Dial Domic [Internet]. 10avr.2019 [cité 12nov.2020];2(1):1-10.
10. De Freitas DG, Gokal R. Sterile peritonitis in the peritoneal dialysis patient. Perit Dial Int. (2005) : 146-51.
11. Yang, C C et al. “Splenic infarction: an unrecognized cause of culture-negative peritonitis in a continuous ambulatory peritoneal dialysis patient.” Clinical nephrology vol. 68,4 (2007) : 262-5. doi:10.5414/cnp68262
12. Nandagopal, L et al. “Sterile peritonitis because of splenic infarction in a patient on peritoneal dialysis: an unusual presentation.” Peritoneal dialysis international : journal of the International Society for Peritoneal Dialysis vol. 33,3 (2013): 339-40. doi:10.3747/pdi.2012.00139
13. Masaki, Chiaki et al. “Splenic abscess diagnosed following relapsing sterile peritonitis in a peritoneal dialysis patient: A case report with literature review.” Seminars in dialysis vol. 34,3 (2021): 245-251. doi:10.1111/sdi.12953
14. Manga, Farhabanu et al. “Acute pancreatitis in peritoneal dialysis: a case report with literature review.” European journal of gastroenterology & hepatology vol. 24,1 (2012): 95-101. doi:10.1097/MEG.0b013e32834d4bcc
15. Osaki, Yosuke et al. “Peritoneal dialysis-associated peritonitis, caused by superior mesenteric artery thrombosis with intestinal necrosis: a case report.” CEN case reports vol. 14,1 (2025): 1-5. doi:10.1007/s13730-024-00894-y
16. Chen, Chih-Wei et al. “Intestinal goblet cell carcinoid presenting with recurrent sterile peritonitis in a patient on peritoneal dialysis: a case report.” BMC nephrology vol. 18,1 62. (2017) doi:10.1186/s12882-017-0477-x
17. Streather, C P et al. “Carcinoma of the kidney presenting as sterile peritonitis in a patient on continuous ambulatory peritoneal dialysis.” Nephron vol. 58,1 (1991) : 121. doi:10.1159/000186395
18. Jobson, V W, and P L Adams. “Endometrial carcinoma diagnosed by examination of peritoneal dialysate.” Obstetrics and gynecology vol. 62,2 (1983) : 264-6.
19. Akimoto, Tetsu et al. “Peritoneal Dialysis and Malignancy: An Experience With a Patient Complicated by Gastric Carcinoma.” Clinical medicine insights. Case reports vol. 12 1179547619835176. (2019) doi:10.1177/1179547619835176
20. Vlahakos, D et al. “Lymphoma-mimicking peritonitis in a patient on continuous ambulatory peritoneal dialysis (CAPD).” Peritoneal dialysis international: journal of the International Society for Peritoneal Dialysis vol. 10,2 (1990) : 165-7.
21. Bargman, J M et al. “Diagnosis of lymphoma in a continuous ambulatory peritoneal dialysis patient by peritoneal fluid cytology.” American journal of kidney diseases: the official journal of the National Kidney Foundation vol. 23,5 (1994) : : 747-50. doi:10.1016/s0272-6386(12)70289-5
22. Delgado-Córdova, Margarita et al. “Non-Hodgkin lymphoma mimicking peritonitis in a patient on peritoneal dialysis.” Nefrologia : publicacion oficial de la Sociedad Espanola Nefrologia vol. 34,5 (2014): 686-7. doi:10.3265/Nefrologia.pre2014.Apr.12386
23. Viray, Paul et al. “Hodgkin’s Lymphoma Diagnosed from Peritoneal Effluent.” Peritoneal dialysis international : journal of the International Society for Peritoneal Dialysis vol. 36,3 (2016): 350-1. doi:10.3747/pdi.2015.00119
24. Sriperumbuduri, Sriram, and Deborah Zimmerman. “Cloudy Dialysate as the Initial Presentation for Lymphoma.” Case reports in nephrology vol. 2018 2192043. 9 Oct. 2018, doi:10.1155/2018/2192043
25. Vigil, Darlene et al. “Noninfectious Cloudy Peritoneal Effluent in a Peritoneal Dialysis Patient with Mantle Cell Lymphoma.” Cureus vol. 10,10 e3413. (2018) doi:10.7759/cureus.3413
26. Vannucchi AM, Kantarjian HM, Kiladjian JJ, et al. A pooled analysis of overall survival in COMFORT-I and COMFORT-II, 2 randomized phase III trials of ruxolitinib for the treatment of myelofibrosis. Haematologica. (2015) : 1139-45. doi:10.3324/
Téléchargements
Soumis
Accepté
Publié
Comment citer
Numéro
Rubrique
Licence
© Charlotte Gabilan 2025

Ce travail est disponible sous la licence Creative Commons Attribution 4.0 International .





